A question that comes up often is whether high Estradiol, early Progesterone, or early/high Spironolactone may stunt or limit good breast development. There are limited studies on this topic; however, here are some resources to help shed some light:
1. High Estradiol
Gender Analysis has a citation for high Estradiol and resultant poor breast development. Source:
https://pubmed.ncbi.nlm.nih.gov/23055547/
. 4425–4426:
These data appear to show that those people who self-medicate with estrogen are more likely to be referred for breast augmentation surgery than those who do not. The duration of estrogen exposure and the duration of estrogen use before attending the GIC (and any subsequent mammoplasties) resonate with the initial finding that self-medication is associated with greater need for breast augmentation. This is consistent with studies on puberty induction in natal girls in whom rapid estrogen exposure was found to lead to premature breast bud fusion and poor breast development (8). Those transwomen who self-medicate with estrogen may be taking too large a dose at initiation to promote appropriate subsequent breast growth, resulting in a poorer final breast outcome. As breast hemicircumference was not measured in this study; it was not possible to determine whether individuals who underwent breast augmentation had objectively smaller breasts. It should be noted, however, that unlike the situation in natal women, breast hemicircumference measurements are limited in their ability to quantify the appearance of breast development in transwomen. The median breast development in transwomen is reported to be 19 cm, which is near natal female norms (2). Despite this fact, 60% of transwomen still present for breast augmentation.
It has been pointed out that reference (8) may be the ONLY reference in any studies related to high Estradiol and premature breast bud fusion. This (8) reference seems to be found again and again on correlation with breast augmentation incidence.
(8) https://link.springer.com/article/10.1186/1750-1172-7-S1-S6
Does DIY (Do It Yourself) HRT (Hormone Replacement Therapy) result in poor breast development?
DIY HRT does not necessarily result in poor or stunted breast development; however, the largest demographic for breast augmentation is in DIY according the same high Estradiol references cited previously.
These data appear to show that those people who self-medicate with estrogen are more likely to be referred for breast augmentation surgery than those who do not. The duration of estrogen exposure and the duration of estrogen use before attending the GIC (and any subsequent mammoplasties) resonate with the initial finding that self-medication is associated with greater need for breast augmentation. This is consistent with studies on puberty induction in natal girls in whom rapid estrogen exposure was found to lead to premature breast bud fusion and poor breast development (8).
Self medicated/DIY guided therapy may not include regular bloodwork/lab monitoring or a thorough understanding of anti-androgen/estradiol interplay and how it may affect premature breast bud fusion.
2. Early Progesterone
TransfeminineScience has a citation for poor breast development with early Progesterone:
https://transfemscience.org/articles/progestogens-suboptimal-breast-dev-excerpts/
17α-Hydroxylase/17,20-Lyase Deficiency
Poor breast development with estrogen therapy has been reported in girls with 17α-hydroxylase/17,20-lyase deficiency and prior exposure to high progesterone levels secondary to the condition has been hypothesized to be responsible for this (Turan et al., 2009; Athanasoulia et al., 2013; Deeb et al., 2015; Çamtosun et al., 2017; Fernández-Cancio et al., 2017; Kardelen et al., 2018). However, this is only a theory and there is no causal evidence that progesterone specifically is responsible.
Progesterone and its Role in Breast Development During Female Puberty (Aly W., 2020):
https://transfemscience.org/articles/p4-breast-dev-puberty/
More about progesterone and breast development:
https://en.wikipedia.org/wiki/Breast_development
There is no well established guideline for the timing of progesterone; however, due to the possibility of limiting breast development, the general rule seems to be waiting 1-2 years after beginning Estradiol hormone treatment (when breast ductal tissue is fully formed). This statement is based upon various citations on online forums from endocrinologists. (not included here as they are scattered)
3. High / Long Term Spironolactone
There are concerns about whether Spironolactone dosage at 100mg or higher per day, for a long period of time, may result in poor breast development. The correlative evidence for this suggestion is poor and are the same reference basis for the high Estradiol premature breast bud fusion:
https://academic.oup.com/jcem/article/97/12/4422/2536439
Compared with other antiandrogens, spironolactone use was significantly higher in those requesting mammoplasty (4.8 vs. 1.8%, P = 0.002).
https://transcare.ucsf.edu/guidelines/feminizing-hormone-therapy
(pg 4), a comment about Spirolactone: The estrogen receptor agonist activity of spironolactone may play a role in reduced breast development due to premature breast bud fusion.
Dr. William Powers states this anecdotally based upon his own observations with transfeminine patients over the years:
Dr. William Powers 2019 v6 presentation:
Here is an interesting TransfeminineScience critique of Dr. Power’s v6 presentation:
https://transfemscience.org/articles/powers-fact-check/
Summary
If you have broken some of these “rules” during transition, keep in mind that the effects of HRT are extremely diverse and individualized. There is no absolute rule that says you will have poor or good breast development. The general rule tends to be that AMAB (Assigned Male at Birth) can usually achieve breasts approximately 1 cup size smaller than cis women relatives; this observation has known exceptions in both directions but is also repeated often in posts online.
Most therapy guidelines will also indicate maximum effect of HRT with breast development is 1-2 years; however, many transfeminine people have posted about long term gains in breast size after 5, or even 10+ years later after starting HRT. These real world posts may be anecdotal, but also offer some evidence contrary to the concept of a 2 year development maximum (which is frankly arbitrary).
Based upon various evidence, minor or major, clinical or correlative; some guidelines to “play it safe” can be established.
1. Dose Estradiol “Low and Slow” and build up gradually over time. This may involve starting with blockers and no Estradiol, or it may involve starting on a lower Estradiol dosage with or without blockers.
Rough outline of equivalent Estradiol dosage:
https://transfemscience.org/articles/e2-equivalent-doses/
If you are going the DIY route, make sure you can build up dose gradually and monitor with labs every 3 months for the first year to ensure your Estradiol range is within general guidelines.
https://www.healthlabs.com/transitional-hormone-wellness-panel
Clinical Guidelines:
https://transfemscience.org/articles/transfem-hormone-guidelines/
2. Avoid Progesterone for the first 1-2 years of Estradiol treatment; until breast ductal tissue has completed development.
3. Avoid Spironolactone as an anti-androgen, or do not take it for the first 3-6 months to help offset the possible premature breast bud fusion effects (a recommendation by Plume for those who may be concerned).
Updates
2021-01-03 Spironolactone Breast Development (anecdotal)
I’ve been keeping an eye open on Reddit for impressive breast development for people who started Spironolactone early and at relatively high doses (100mg or higher). I’ve seen at least 2 confirmed cases of good breast development on Spironolactone early and for long periods of time. Obviously this isn’t a nail in the coffin as people vary dramatically, but it certainly points to Spironolactone not being a deal breaker for good breast development in an absolute sense.
2021-01-10 Survey on Reddit
Not a big sample set, but here are the survey results from a post on Reddit I did:
I’ve been looking into Spiro and poor breast development studies and it’s all very limited information. It occurred to me that perhaps the Reddit trans community could shed some light. There appears to be a statistical correlation between the use of Spiro and poor breast development:
https://academic.oup.com/jcem/article/97/12/4422/2536439
If you have: 1) used Spiro 100mg or greater 2) for 6 months or greater and 3) started Spiro within the first 2 months of taking Estradiol, and 4) have been taking Estradiol for 2 years or greater; please answer this poll to help out the whole community and perhaps shed a little more light into this correlation. Thank you!
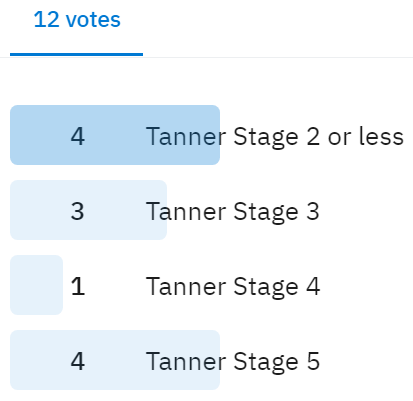
Although there are only 12 votes cast, Spironolactone continues to appear as though it is not a deal breaker for good breast development. I would love to see a more successful survey for this question if anyone can post it and let me know the results to post for everyone.
The notion that high initial estradiol dosage would limit breast-growth is also supported by this mice study:
https://sci-hub.se/10.1210/endo-28-1-53
I’m freaking out a little bit because I boosted my estradiol dose so high within less than a year on it (successfully convinced my doctor to boost me to 200mcg patches and 2mg progynova oral as I’d read crap online that high estrogen was VERY GOOD ACTUALLY and hadn’t come across any of this material about “low and slow” being the best approach for development…)
I’m currently bringing my dosage back down again (I’m also on cypro, but a very low dose, like 12.5 a week) and just desperately praying that I haven’t screwed myself over with my misinformed anxious behaviour…THIS INFORMATION NEEDS TO BE MORE READILY AVAILABLE GOD DAMMIT!! THE GIRLS NEED TO KNOW!!!